
Clinical and echographic characteristics of women with threatened miscarriages and retrochorial hematomas in the Lugansk region, Ukraine
20 August 2019
RESEARCH ARTICLE
Clinical and echographic characteristics of women with threatened miscarriages and retrochorial hematomas in the Lugansk region, Ukraine
Iryna Romanenko1*
1Ukrainian Scientific and Practical Center for Endocrine Surgery, Transplantation of Endocrine Organs and Tissues of the Ministry of Health of Ukraine, Kiyv, Ukraine.
Corresponding author:
Iryna Yurііvna Romanenko, PhD, assoc. prof.
Department of reproductive medicine and surgery
Ukrainian Scientific and Practical Center for Endocrine Surgery, Transplantation of Endocrine Organs and Tissues of the Ministry of Health of Ukraine, Kyiv, Ukraine, zip code 01021
e -mail: iryna.roman2017@gmail.com
Short title: Retrochorial hematomas and threatened miscarriages
What is not known yet, about the topic
The risk profile of the imminence of spontaneous abortion in pregnant women in the first trimester of pregnancy with retrochorial hematoma is not fully elucidated. The causes leading to the formation of the retrochorial hematoma are also insufficiently studied.
Research hypothesis
A number of risk factors favor the appearance of retrochorial hematoma, which in turn becomes an early marker of placental failure and imminence of spontaneous abortion in the first trimester of pregnancy.
Article’s added novelty on this scientific topic
Reproductive losses, chronic inflammatory diseases of the uterine annexes, anamnesis of sexually transmitted infections should be considered risk factors for the development of retrochorial hematoma in the event of a subsequent pregnancy. Retrochorial hematoma, in turn, is an early clinical marker of placental insufficiency, which increases the risk of early and late complications of pregnancy.
ABSTRACT
Introduction. The retrochorial hematoma (RCH) is the most common cause of bleeding in the first trimester of pregnancy. RCH is diagnosed in 4-22% of the number of all pregnancies during the ultrasound examination in the first trimester. According to researchers, pregnancy with RCH often ends with miscarriage, patients with RCH having a higher risk of developing maternal and neonatal complications. The purpose of this research was to study the clinical, laboratory and echographic characteristics of women in the first trimester of pregnancy with a threatened miscarriage (TM) and the RCH with the aim to improve treatment and preventive measures and to prevent obstetric and perinatal complications in such women.
Material and methods. The study included 22 women in the first trimester with TM and RCH, living in the Lugansk region (group I). The control group consisted of 32 pregnant women with uncomplicated obstetric anamnesis, physiological course of pregnancy, a similar gestational period of pregnancy and no pathological changes found at the Ultrasound examination (USЕ) (group II). A comprehensive clinical, laboratory and ultrasound examination was carried out. Results. In women in the first trimester of pregnancy with TM, RCH was noted in 16.42%. The presence of RCH was accompanied by a manifestation of TM in the first trimester in all the women under examination. History of reproductive loss (spontaneous abortion and missed miscarriage), anamnesis of chronic inflammatory diseases of the uterine annexes and sexually transmitted infections were significantly more frequent in women with RCH – 2.17, 2.1, 2.4 and 2.9 times higher, respectively. Pregnant women with RCH were more predisposed to the development of vaginal microbiota, such as non-specific vaginitis and bacterial vaginosis, 2.4 and 1.7 times, respectively. The presence of the RCH had an adverse effect on the second trimester: the pregnant women from group I had a higher incidence of TM, cervical incompetence, placenta praevia – 8.74, 22.73 and 8.74 times, respectively. In pregnant women with RCH in the first trimester, the pre-eclampsia prevalence rate did not differ from that of the control group, while the frequency of preterm labor was 4.36 times higher. Cases of placental abruption, abnormal delivery and premature rupture of fetal membranes before 37 weeks of gestation were noted only in group I.
Conclusions. The presence of RCH contributes to the identification of the pregnant women who are at high risk of development of gestational complications, with the aim of applying proper prophylactic measures and timely treatment.
Keywords: pregnancy, threatened miscarriage, retrochorial hematoma.
INTRODUCTION
The retrochorial hematoma (RCH) is the most common cause associated with haemorrhage in the first trimester of pregnancy [1, 2, 3]. During the first trimester screenings, RCH is diagnosed in 4-22% of pregnancies [4, 5]. According to the researchers, pregnancies with RCH end in spontaneous abortions in a high percentage of cases [3, 6, 7]. Patients with RCH have a higher risk of developing maternal and neonatal complications: delayed fetal growth, stillbirth, premature rupture of fetal membranes, premature placental abruption, premature delivery, fetal distress, meconium aspiration [6-10]. Due to the relatively high frequency of RCH and its negative effect on the evolution of pregnancy, the problem of perinatal complications prevention among pregnant women with RCH is relevant [4]. Purpose of the study: to point out the clinical, laboratory and ultrasound characteristics of women in the first trimester of pregnancy with threatened miscarriage and retrochorial hematoma for enhancing the therapeutic and preventive methods and for the prophylaxis of obstetric and perinatal complications in such women.
MATERIAL AND METHODS
After examining 134 pregnant women in the first trimester of pregnancy, hospitalized with threatened miscarriage in hospitals from Rubezhnoye and Lisichansk, Lugansk region, in 2015-2017, retrochorial hematomas were detected in 22 women, forming the study group. The control group (group II) consisted of 32 pregnant women with uncomplicated medical history, physiological evolution of pregnancy, same gestational age and without pathological ultrasound changes. Prior to the start of the study, each respondent signed the informed consent for the diagnosis, treatment, and processing of personal data. The inclusion criteria of the study group were the following: the symptoms of threatened miscarriage, the gestational period corresponding to the first trimester of pregnancy, and the presence of retrochorial hematomas on the ultrasound.
The surveillance and clinical examination of women were carried out in accordance with the recommendations established in the orders of the Ministry of Health of Ukraine on July 15, 2011, no. 417 “On the organization of ambulatory obstetric and gynecological care in Ukraine” and on November 3, 2008 – no. 624 (Clinical Protocol “Pregnancy loss”).
All the pregnant women underwent a detailed clinical and laboratory examination (medical history taking, clinical and obstetrical examination, clinical and biochemical blood test, coagulation tests, study of β-hCG and PAPP-A placental proteins, urinalysis, microscopic and bacteriological examination of vaginal and cervical secretions), ultrasound of the pelvic organs in the first trimester, fetal ultrasound and Doppler ultrasound in the second and third trimesters of pregnancy.
Categorical type data are presented as absolute and relative values. Ordinal data are presented as median (Me) with the 25-75% percentile interval (Q1-Q3). The normality of the data distribution was tested by the Shapiro-Wilk criterion. Significant differences were evaluated using the Mann-Whitney non-parametric assay for independent samples. The statistical significance of the associations between qualitative indicators of the frequency of occurrence of factors was evaluated using the Pearson χ2 test or Fisher`s exact test. A p<0.05 was considered statistically significant. Statistical data analysis was performed using the SPSS 17.0 software.
RESULTS
The mean age of the women from group I was 26 (22-33) years and from group II – 27.5 (23-32) years. Most of the patients were 20-30 years old – 14 (63.64%) and 22 (68.75%), respectively, i.e. they were part of the active and working population. Most women were in a registered marriage – 19 (86.36%) and 27 (84.36%), respectively.
The BMI was 24.06 (20.90-30.41) kg/m2 in the study group and 21.61 (19.71-25.91) kg/m2 in the control group (p=0.245). The family thrombotic history was uncomplicated in both groups.
The mean age of the menarche in both the examined groups was 13.00 (12.00-14.00) years. In pregnant women, the following somatic diseases were registered: respiratory diseases – 4 (18.18%) and 5 (15.63%) women, respectively, signs of urinary tract diseases – 2 (9.01%) and 1 (13%), 1st–2nd degree thyroid gland hyperplasia with euthyroidism – 3 (13.64%) and 1 (3.13%), pollinosis – 3 (13.64%) and 3 (9.38%) women, respectively.
History of spontaneous abortion, missed miscarriage, was recorded much more frequently in pregnant women from the group I (Table 1).
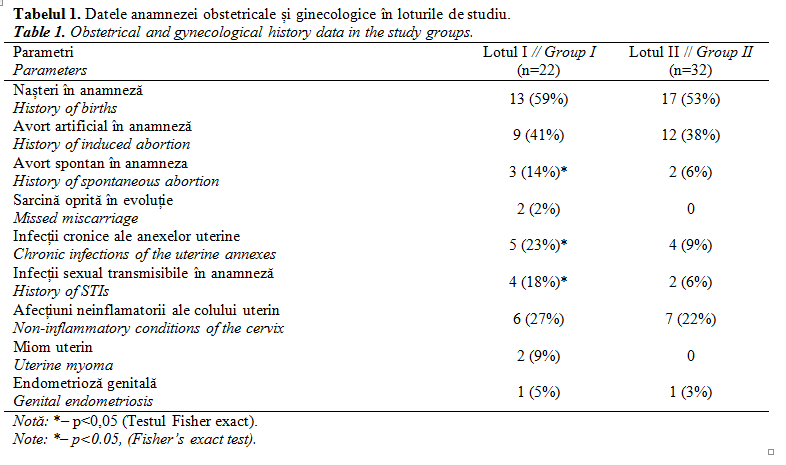
According to the data from the table, chronic inflammatory diseases of the uterine annexes, sexually transmitted infections (STIs) and uterine fibroids occurred significantly more frequently in the pregnant women from the study group, compared to the pregnant women from the control group. There was no significant statistical difference in the incidence of non-inflammatory cervical diseases and genital endometriosis in both the groups.
The analysis of hemostasis parameters revealed significant differences for the prothrombin index (PI): in the 1st group, PI (%) was 84.00 (82.00-88.00)%, in the 2nd group – 89.50 (87.00-97.50)% (p=0.016), which may indicate hypocoagulation in pregnant women with RCH. There was a trend towards high fibrinogen values in group I compared to group II: 3.44 (3.33-3.55) g/l and 3.2 (3.02-3.54) g/l, respectively (p=0.056).
After performing the biochemical screening in the first trimester, including chorionic gonadotropin (β-hCG) and pregnancy-associated plasma protein (PAPP-A), the placental protein concentration was not significantly different. The PAPP-A, multiple of the median (MoM) indicator was 1.50 (0.63-2.01) in group I, and 1.22 (0.77-1.69) in group II (p=0.078); the β-hCG, MoM indicator constituted 1.33 (0.83-1.43) and 1.42 (0.95-1.91), respectively (p=0.24).
Upon admission to hospital, all the pregnant women were subjected to an ultrasound; the data are shown in Table 2.
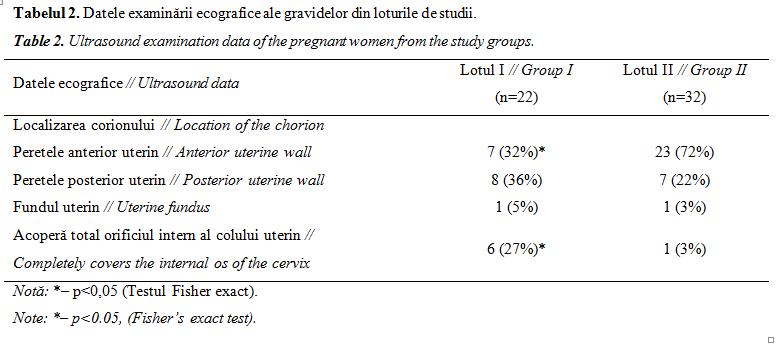
Based on the presented data, the most common location of the chorion among the pregnant women from the control group is on the anterior wall (71.88%), while the pregnant women from group I enlisted the location on the anterior wall of the uterus in 31.82%, the posterior wall of the uterus in 36.36%, the uterine fundus in 4.55% and the endocervix in 27.27% of the cases. Placenta previa was found significantly more frequently in the pregnant women from group I (p=0.018).
Retrochorial haematomas had the volume of 1.50 (0.34-1.61) cm3, the corpus localization was recorded in 15 (68.18%) cases, the supracervical localization – in 7 (31.82%) cases. The RCH were described as unorganized in 10 (45.45%) cases, with signs of organization in 8 (36.36%) cases, and organized in 4 (18.18%) cases.
Upon admission, all the pregnant women from group I who were in outpatient conditions and the pregnant women from group II were subjected to the bacterioscopic and bacteriological examination of the vaginal discharge, which made it possible to determine the status of the microbiota in the study groups (Table 3).
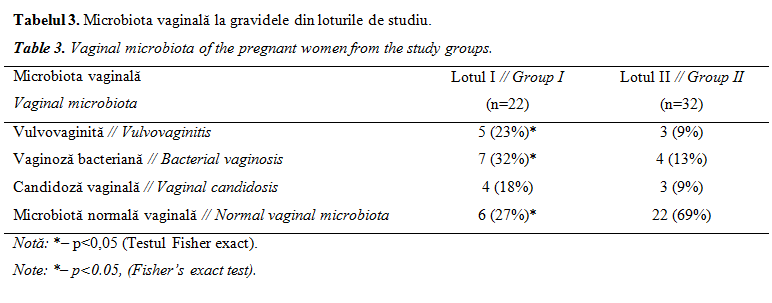
In the study group I, vulvovaginitis and bacterial vaginosis were detected much more frequently in the control group – 22.73% and 31.82%, respectively, compared to the normal vaginal microbiota – 68.75%.
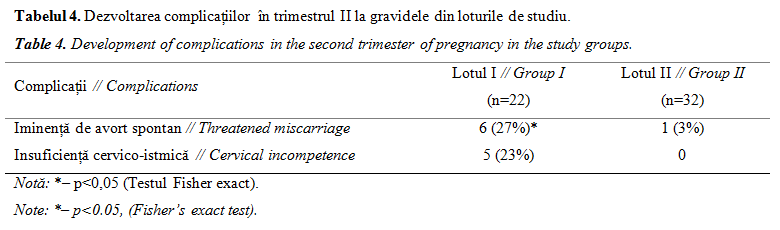
Analyzing the subsequent course of pregnancy in women with RCH in the first trimester, it may be noticed that they were more likely to experience threatened miscarriage and cervical incompetence in the second trimester (Table 4).
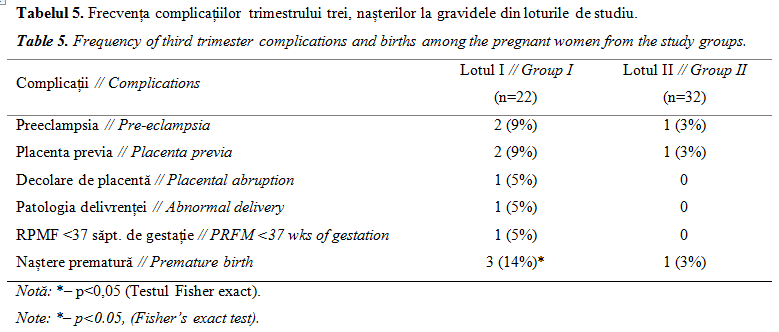
 The third trimester and pregnancy analysis in pregnant women with RCH showed that the frequency of pre-eclampsia and placenta praevia did not differ from the control group, while the rate of premature delivery was higher (p=0.038). Cases of placental abruption, abnormal labor and premature rupture of fetal membranes (PRFM) before 37 weeks of gestation were recorded only in the main group (Table 5).
The third trimester and pregnancy analysis in pregnant women with RCH showed that the frequency of pre-eclampsia and placenta praevia did not differ from the control group, while the rate of premature delivery was higher (p=0.038). Cases of placental abruption, abnormal labor and premature rupture of fetal membranes (PRFM) before 37 weeks of gestation were recorded only in the main group (Table 5).
DISCUSSION
In our study, retrochorial hematoma was detected in 16.42% of the women in the first trimester of pregnancy with threatened miscarriage, which corresponds to the data of Xiang L. et al. [3], but exceeds Peixoto A. et al. data [4]. The presence of RCH resulted in threatened miscarriage in the first trimester among all the women examined.
Statistically significant differences in the prevalence of extragenital disorders in pregnant women from both groups were not found, suggesting that these somatic diseases are not an initial background for RCH development. History of reproductive losses (spontaneous abortion and missed miscarriage), anamnesis of chronic inflammatory diseases of the uterine annexes, sexually transmitted infections are significantly more common in women with RCH (2.17, 2.1, 2.4 and 2.9 times, respectively), which allows us to consider them as a risk factor for RCH development in the event of a later pregnancy. Our data correspond to Soldo V. et al. [5], but are partly contrary to those of Yamada T. et al. [11].
No significant differences were found for BMI in the examined lots, which confirms Peixoto A. et al. opinion [4]. When analyzing hemostasis parameters, a significant decrease towards the lower level of baseline PI values in group I was noted, which may indicate a tendency towards hypocoagulation in pregnant women with RCH. There was an inclination towards high levels of fibrinogen in group I, which did not refute the results of Hackney D. et al. [1]. During the first trimester biochemical screening, including the determination of β-hCG and PAPP-A, the placental protein concentration in the examined groups was not significantly different.
According to our study data, vaginal microbiota alteration was significantly more common in pregnant women with RCH: non-specific vaginitis, bacterial vaginosis were 2.4 and 1.7 times more common, which is consistent with the results of Yamada T et al. [11].
The results of our study have shown that the presence of the retrochorial hematoma negatively affects the course of the second trimester. In pregnant women from group I, a higher incidence of threatened miscarriage, cervical incompetence and placenta praevia was observed – 8.74, 22.73 and 8.74, respectively. An informative method for estimating the pregnancy evolution is the ultrasound.
In our study, it was shown that the frequency of pre-eclampsia, placenta praevia in pregnant women with RCH in the first trimester did not differ from the control group, while the preterm birth rate was 4.36 times higher. The cases of placental abruption, the abnormal delivery, premature rupture of fetal membranes (PRFM) before 37 weeks of gestation were observed only in the main group, corresponding to the data of Tuuli M.G. et al. [7], but not agreeing with the opinions of Peixoto A. et al. [4] and Biesiada L. et al. [12].
CONCLUSIONS
Among the women in the first trimester of pregnancy with threatened miscarriage, the retrochorial hematoma occurs in 16.42% of cases. History of pregnancy loss (spontaneous abortion and missed miscarriage), anamnesis of chronic inflammatory diseases of the uterine annexes and sexually transmitted infections should be considered as risk factors for the development of RCH in the event of a subsequent pregnancy.
The retrochorial hematoma is an early clinical marker of placental insufficiency, increasing the risk of early and late complications of the pregnancy: threatened miscarriage, cervical incompetence, premature birth, placental abruption, abnormal delivery, premature rupture of fetal membranes. The presence of retrochorial hematoma allows the identification of pregnant women at high risk for the development of gestational complications in order to apply prophylactic and treatment methods in a timely manner.
Declaration of conflicting interests
The author states the lack of conflicts of interest in the preparation of this article.
REFERENCES
- Hackney D., Miller R., Pressman E., Francis C., Simhan H. Vaginal bleeding in early pregnancy and circulating markers of thrombin generation. J. Matern. Fetal Neonatal Med., 2012; 25 (8): 1479-1482. doi:10.3109/14767058.201644602.
- Hackney D., Glantz J. Vaginal bleeding in early pregnancy and preterm birth: systemic review and analysis of heterogeneity. J. Mat. Fetal Neonat. Med., 2011; 24: 778–786.
- Xiang L., Wei Z., Cao Y. Symptoms of an intrauterine hematoma associated with pregnancy complications: a systematic review. PLoS ONE, 2014; 9(11): e111676.
- Peixoto A., Caldas T., Petrini C., Romero A., Júnior L., Martins W., Araujo Júnior E. The impact of first-trimester intrauterine hematoma on adverse perinatal outcomes. Ultrasonography, 2018; 37(4): 330-336. doi: 10.14366/usg.18006.
- Soldo V., Cutura N., Zamurovic M. Threatened miscarriage in the first trimester and retrochorial hematomas: sonographic evaluation and significance. Clin. Exp. Obstet. Gynecol., 2013; 40 (4): 548-50.
- Kyser K. Meta-analysis of subchorionic hemorrhage and adverse pregnancy outcomes. Proceedings in Obstetrics and Gynecology, 2012; 2 (4): 4.
- Tuuli M., Norman S., Odibo A., Macones G., Cahill A. Perinatal outcomes in women with subchorionic hematoma: a systematic review and meta-analysis. Obstet. Gynecol., 2011; 117 (5): 1205-12. doi: 10.1097/AOG.0b013e31821568de.
- Chhabra A., Lin E. Subchorionic hemorrhage imaging. Medscape.com: website. – WebMD LLC, 1994-2016. http://emedicine.medscape.com/article/404971-overview [Accessed on: 19.05.2015].
- McPherson J., Odibo A., Shanks A., Roehl K., Macones G., Cahill A. Adverse outcomes in twin pregnancies complicated by early vaginal bleeding. Am. J. Obstet. Gynecol., 2013; 208 (1): 56.e1-5. doi: 10.1016/j.ajog.2012.10.875.
- Palatnik A., Grobman W. The relationship between first-trimester subchorionic hematoma, cervical length, and preterm birth. Am. J. Obstet. Gynecol., 2015; 213 (3): 403.e1-4. doi: 1016/j.ajog.2015.05.019.
- Yamada T., Atsuki Y., Wakasaya A., Kobayashi M., Hirano Y., Ohwada M. Characteristics of patients with subchorionic hematomas in the second trimester. J. Obstet. Gynaecol. Res., 2012; 38 (1): 180-4. doi: 10.1111/j.1447-0756.2001665.x.
- Biesiada L., Krekora M., Krasomski G. Subchorionic hematoma as a risk factor of pregnancy and delivery in women with threatening abortion. Ginekol. Pol., 2010; 81 (12): 902-6.