IMAGES FROM CLINICAL PRACTICE
20 August 2019
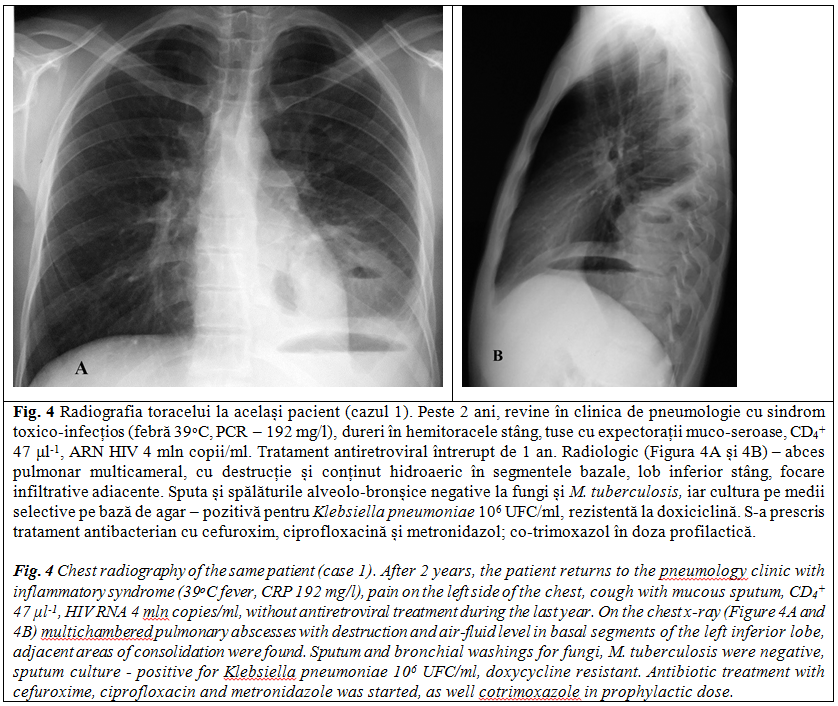
Multiple lung involvements – a landmark in immunocompromised patient
Victor Botnaru1, Doina Rusu1,2, Eugenia Scutaru1*, Dumitru Chesov1
1Discipline of pneumology and alergology, Department of internal medicine, Nicolae Testemitanu State University of Medicine and Pharmacy, Chisinau, Republic of Moldova.
2Phthisiopneumology Institute „Chiril Draganiuc”, Chisinau, Republic of Moldova.
Corresponding author:
Eugenia Scutaru, assistant professor
Discipline of pneumology and alergology
Department of internal medicine
Nicolae Testemitanu State University of Medicine and Pharmacy
165, Stefan cel Mare si Sfant bd., Chisinau, Republic of Moldova, MD-2004
e-mail: evghenia.scutaru@usmf.md
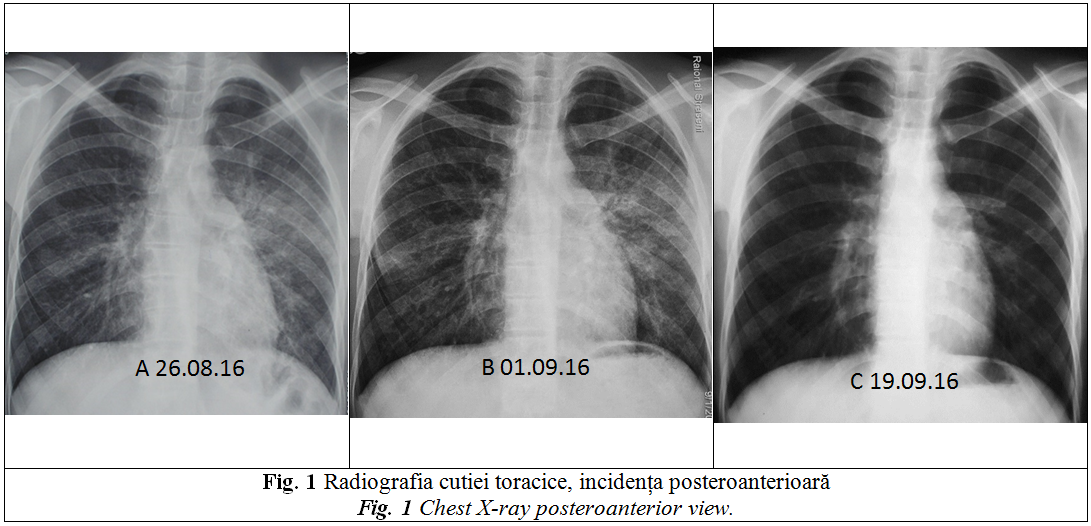
A 25 years old nonsmoker man, known as migrant worker, was admitted for dyspnea (mMRC II), low fever, cough with minimal mucous sputum (for 2 weeks) and weight loss (15 kg over previous 2 months). Seven days prior current admission he was diagnosed with left side bronchopneumonia and treated with combined antibiotics (ceftriaxone and levofloxacin). On treatment no clinical improvement and even radiological worsening, was observed (Figure 1A, 1B).
On admission, physical examination revealed a body mass index of 17 kg/m2, respiratory rate – 18 rpm, heart rate – 94 bpm; blood pressure – 110/80 mmHg, SpO2 – 89% on room air and vesicular breathing on both hemithoraces.
The blood tests shown lymphopenia (lymphocytes 2.6×103µl-1) and increased level of C reactive protein (CRP) – 18 mg/l. His HIV test was positive and CD4+ count was extremely low – 3 μl-1. Pulmonary functional tests shown a mixed ventilatory dysfunction (FEV1 – 66%, FVC – 59%, FEV1/FVC – 96, RV – 171%, TLC – 94% and reduced alveolar-capillary diffusion (DLCO – 50%).
QUESTIONS:
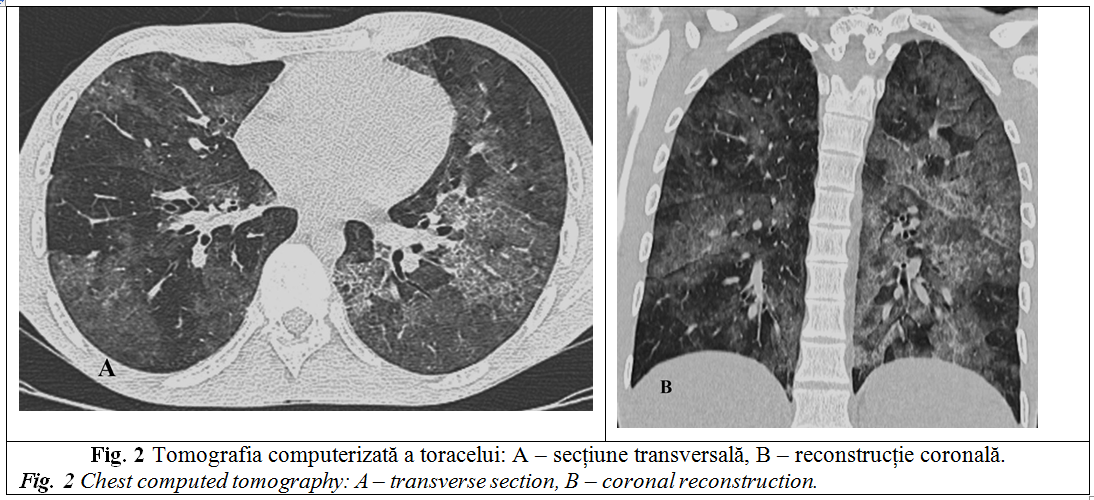
- What are the changes on chest radiography (Figure 1A) and chest CT images (Figure 2)?
- Considering patient history and imaging, which is the most likely diagnosis?
- What additional tests would you suggest for confirmation of the diagnosis?
- Which other imaging patterns are suggestive for this disease?
ANSWERS:
- The chest radiography shows (Figure 1A) bilateral reticulonodular opacities, of moderate intensity, predominantly in the left lung, prominent pulmonary artery, probably due to thoracic scoliosis (pulmonary blood pressure 30 mmHg). Chest CT (Figure 2) confirms interstitial lesions – areas of ground glass alternate with normal lung parenchyma – mosaic distribution.
- Pneumocystis jiroveci pneumonia (PCP), a condition that often defines AIDS, occurs when the number of T helper (CD4+) is less than 200 µl-1 [1]. The immune response to P. jiroveci infection involves the interaction of T-lymphocytes, alveolar macrophages, neutrophils, which facilitate eradication of the infection. Proliferation of the pneumocystis is associated with production of an alveolar exudate, followed by interstitial pneumonitis. With the progression of the disease, the trophozoites and cellular cells accumulate in the alveoli leading to their obliteration. There is an impairment of surfactant synthesis and decrease in gas diffusion causing respiratory failure.
- PCP diagnosis is confirmed by microscopy of bronchioloalveolar lavage or induced sputum, with detection of cystic forms (Gomori-Grecott stains with blue toluidine or calcofluor white for cysts) or fungal trophozoites (Wright-Giemsa, Papanicolau or Gram-Weigert stains), the sensitivity ranges between 50-90% [1, 5]. There are also other diagnostic tests confirming P. jiroveci infection: sputum smear immunofluorescence with monoclonal antibodies; serological markers as S-adenosylmethionine and (1R3)-b-D-glucan [2-4]; polymerase chain reaction techniques (PCR).
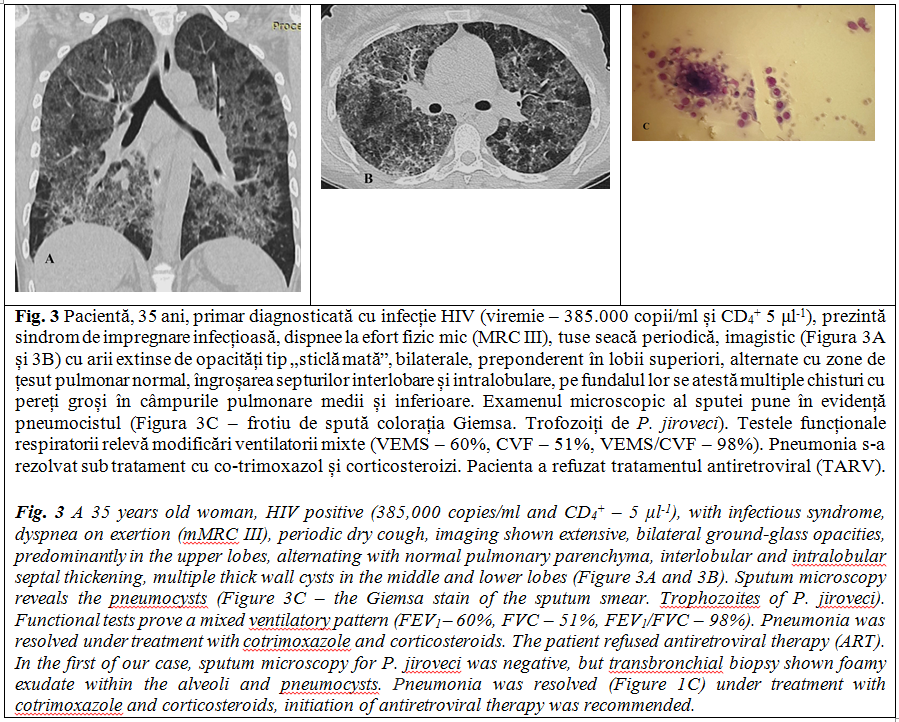
- PCP imaging is various. The most common patterns are: nodular (multiple nodules, merging into homogenous areas of consolidation alternating with normal pulmonary parenchyma – mosaic attenuation pattern); "ground glass" opacities (Figure 2) (diffuse bilateral homogeneous attenuation, on which the vascular and bronchial structures are visualized, with predominantly upper lobes and apical segments of the lower lobes involvement); interstitial pattern characterized by septal and nonseptal linear opacities associated or not with ground glass areas and consolidations). Cavities (pneumatoceles) or cysts (Figure 3A, 3B), mediastinal and hilar lymphadenopathy, excavated nodules are less commonly observed.
Pneumonia is a common complication in patients with severe immunodeficiency, especially HIV-infected patients develop pneumonia in over 50% of cases [6]. P. jiroveci is a unicellular ubiquitous fungus (formerly considered protozoar), has an unique tropism for lung parenchyma, being an alveolar pathogen. Pneumonia with P. jiroveci, often defines AIDS in HIV-infected patients, usually occurs when the number of T helper (CD4+) is less than 200 μl-1.
Commonly PCP symptoms have a subacute onset with progressive dyspnea, dry cough and fever. Significant weight loss and respiratory failure with rapid deterioration of the general condition are also frequently seen in AIDS patients with PCP [5]. However, up to 7% of these patients can be asymptomatic, some of them have mildly expressed radiological changes (radiological-negative pneumonia caused by P. jiroveci is largely recognized in immunocompromised hosts) [6].
In cases with T-helper (CD4+) counts below 200 μl-1, pulmonary infections are more commonly caused by S. viridans, enterococci, hospital acquired gentamicin resistant strains, Gram negative bacteria, P. jiroveci, Aspergillus, mycobacteria, viruses.
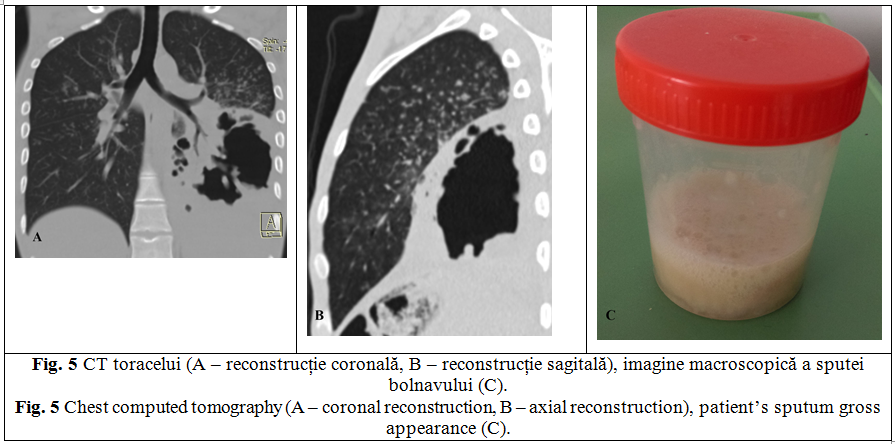
The patient was discharged with improved clinical symptoms and normalized CRP serum level. It was recommended to continue combined antibiotic therapy (amoxicillin, levofloxacin) in outpatient and to restart ART. He returns after 4 months with dyspnea on exertion (mMRC III), cough with purulent sputum <50 ml/24 hours (Figure 5C), weight loss (8 kg in 2 weeks), night sweating, marked asthenia and pollakiuria. Chest HRCT (Figures 5A, 5B) revealed a partially drained, large pulmonary abscess (10×7×10 cm), in the lower left lobe, multiple nodular opacities (up to 4 mm in diameter), with predominantly centrilobular distribution in the left upper lobe, and entire right lung. Sputum tests for M. tuberculosis (microscopy, Xpert MTB/Rif, culture on liquid media) and fungi were negative. However, Mycobacterium fortuitum, was confirmed by line probe assay (LPA) in one of the sputum samples. Missing confirmation of M. fortuitum infection in other sputum samples pushed the diagnosis to that of pulmonary tuberculosis based on clinical and imaging criteria (large lower left lobe cavity – caverna magna and signs of bronchiolitis). Tuberculosis treatment with rifampicin, isoniazid, ethambutol, pyrazinamide and levofloxacin with body mass adjusted doses, was initiated.
In HIV positive patients with CD4+ <200 μl-1 a variety of opportunistic infections can occur. Etiological diagnosis of interstitial and cavitary imaging lesions is often challenging and imply a large list of differential diagnosis including mycotic, bacterial tuberculosis infections and others.
Declaration of conflicting interests
Nothing to declare.
REFERENCES
- Shibata S., Kikuchi T. Pneumocystis pneumonia in HIV-1-infected patients. Respir. Investig., 2019.
- Kanne J., Yandow D., Meyer C. Pneumocystis jiroveci pneumonia: high-resolution CT findings in patients with and without HIV infection. American Journal of Roentgenology, 2012; 198 (6): W555-W561.
- Luks A., Neff M. Pneumocystis jiroveci pneumonia. Respir. Care, 2007; 52 (1): 59-63.
- Thomas C., Limper A. Pneumocystis pneumonia. New England Journal of Medicine, 2004; 350 (24): 2487-2498.
- Salzer H. et al. Clinical, diagnostic, and treatment disparities between HIV-infected and non-HIV-infected immunocompromised patients with Pneumocystis jirovecii pneumonia. Respiration, 2018; 96 (1): 52-65.
- Carmona E., Limper A. Update on the diagnosis and treatment of Pneumocystis pneumonia. Therapeutic Advances in Respiratory Disease, 2011; 5 (1): 41-59.